





People with type 2 diabetes mellitus (DM2) have a higher prevalence of frailty compared to those without DM2. However, there is a lack of consensus on the diagnosis and clinical management of frail individuals with DM2.
ObjectivesThis study aims to identify limitations and current needs in the use of the frailty concept in PCDM2 (people with DM2), as well as define and evaluate the dimensions that should be included in its routine clinical assessment.
MethodsA multidisciplinary team of eight health professionals from different hospitals in Spain participated in a process based on the nominal group technique.
ResultsThe study identified eight limitations in the assessment of frailty in PCDM2, categorized by importance, and 10 unmet needs related to the diagnosis and follow-up of the disease. Additionally, seven dimensions were identified that should be included in the definition of frail individuals with DM2, prioritized by importance and novelty.
ConclusionsThis article aims to increase knowledge and usage of the frailty concept in individuals with DM2 within the medical community. It also suggests the potential for future projects to develop a consensus definition of frailty tailored to this specific group.
Las personas con diabetes mellitus tipo 2 (DM2) tienen una prevalencia de fragilidad que se estima entre 3 y 5 veces mayor que aquellos que no la padecen, sin embargo, no existe un consenso claro sobre el diagnóstico y manejo clínico durante el itinerario de la persona frágil con DM2.
ObjetivosEl objetivo principal de este estudio es identificar las limitaciones y necesidades actuales en el uso del concepto de fragilidad en personas con DM2 (PCDM2), así como definir y evaluar, según su importancia y novedad, las dimensiones que podrían incluirse en su valoración clínica de rutina.
MétodosSe llevó a cabo un proceso basado en la técnica de grupo nominal con la participación de un equipo multidisciplinario de 8 profesionales de la salud que trabajan en diferentes hospitales de España.
ResultadosSe identificaron y clasificaron según su importancia un total de 8 limitaciones en la evaluación de la fragilidad en PCDM2, así como 10 necesidades no satisfechas relacionadas con el diagnóstico y seguimiento de la enfermedad. Además, se identificaron 7 dimensiones que consideramos que deben incluirse en la definición de la persona frágil con DM2, ordenadas por importancia y novedad.
ConclusionesEl presente artículo podría lograr aumentar el conocimiento y uso en la comunidad médica del concepto de fragilidad en la persona con DM2 y desembocar en un futuro proyecto que logre realizar, de manera consensuada, una definición de fragilidad adaptada a este colectivo.
Frailty is a dynamic, complex syndrome and the risk of presenting with it increases with age.1 It is characterized by increasing the individual’s vulnerability to external factors and the risk of health problems.1 Although frailty tends to be related to physical and performance status,1 there is growing evidence that it could be defined in a multidimensional manner, encompassing physiological, psychological, cognitive, nutritional, and social aspects.2–4 Due to the complexity of evaluating frailty and the lack of a standard for diagnosis, comparing results from different studies is a great challenge.3,5
Individuals with type 2 diabetes mellitus (DM2) are estimated to have a prevalence of frailty between three to five times greater than those without DM2.6,7 In Spain, frailty syndrome affects 14.6% of individuals with DM2 (IWDM2), which is present in 13.8% of the Spanish population and increases in frequency in advanced age.8
The coexistence of both conditions has negative effects on health, psychosocial wellbeing, and quality of life, which in turn increases healthcare costs for IWDM2 and frailty.9–11 The relationship between frailty and DM2 is complex. There is significant evidence that DM2 contributes to the onset and increases the severity of frailty.12,13 Hyperglycemia is related to its onset and levels of glycated hemoglobin are associated with its severity.14 The vascular complications of DM2 are also associated with inactivity and physical and cognitive decline, which may lead to the onset of frailty.15
Appropriate treatment aims for IWDM2 vary according to frailty.16,17 IWDM2 and frailty are more prone to hypoglycemia and more vulnerable to its consequences, such as falls, fractures, hospitalizations, cardiovascular episodes, and mortality.16 The identification of frailty and its ongoing assessment may help avoid related complications and achieve better treatment adjustment, improving safety, adherence, and care for individuals with frailty and DM2.18,19
Despite the association between and importance of both conditions and the significant advances on this matter in Spain, there is still no clear consensus on the diagnosis and clinical management of individuals with frailty and DM2. This study aims to identify the current limitations and needs on the use of the concept of frailty in IWDM2 and define and evaluate the dimensions that could be included in its routine clinical assessment, considering their importance and novelty.
MethodsParticipantsThe study was conducted by a scientific committee (SC) comprising eight members with different medical specialties, including four primary care physicians, two endocrinologists, and two internal medicine physicians (the authors of this article). The Anima Strategic Consulting medical agency participated in the conduct of the project and facilitated meetings and communication between SC members.
PhasesThe project consisted of four phases, which are described in Fig. 1. In phase 1, the project was designed and a literature search was conducted to compile relevant information on the management and use of the concept of frailty in IWDM2. In phase 2, an online questionnaire was distributed to the SC and the responses were gathered and summarized. In phase 3, a meeting of the SC was held in which the questionnaire responses were presented and classified. The key issues on frailty in IWDM2 were discussed. Phase 4 consisted of writing the manuscript, which included an abstract and the results of the project.
Nominal group technique
Nominal group technique (NGT) is used to ensure equitable participation among all members and promote expressing opinions during the project.20,21 In the first step, the SC created a series of questions which were distributed through an online questionnaire (Table 1). Each SC member responded to the questionnaire individually. Later, the responses were grouped in order to be discussed in an online meeting that took place on February 1, 2023. During the meeting, the ideas generated were debated and prioritized by means of voting using the Mentimeter tool (https://www.mentimeter.com). This tool allowed for anonymous online voting and immediate viewing of the results. Thanks to NGT, equitable representation of all participants was achieved and individual influence on the group’s decisions were limited.20,21
Questionnaire created in phase 2.
| How would you define an individual with frailty and DM2? |
| What needs do you consider an individual with frailty and DM2 to have and why? |
| What types of individuals with frailty and DM2 or patient profiles do you come across in your daily practice? |
| What main limitations would you highlight in the assessment of frailty in DM2? |
| How do you evaluate frailty in an individual with DM2 in your consultation? |
| What variables must be considered (which are not considered at present) in order to define frailty in an individual? |
DM2: type 2 diabetes mellitus.
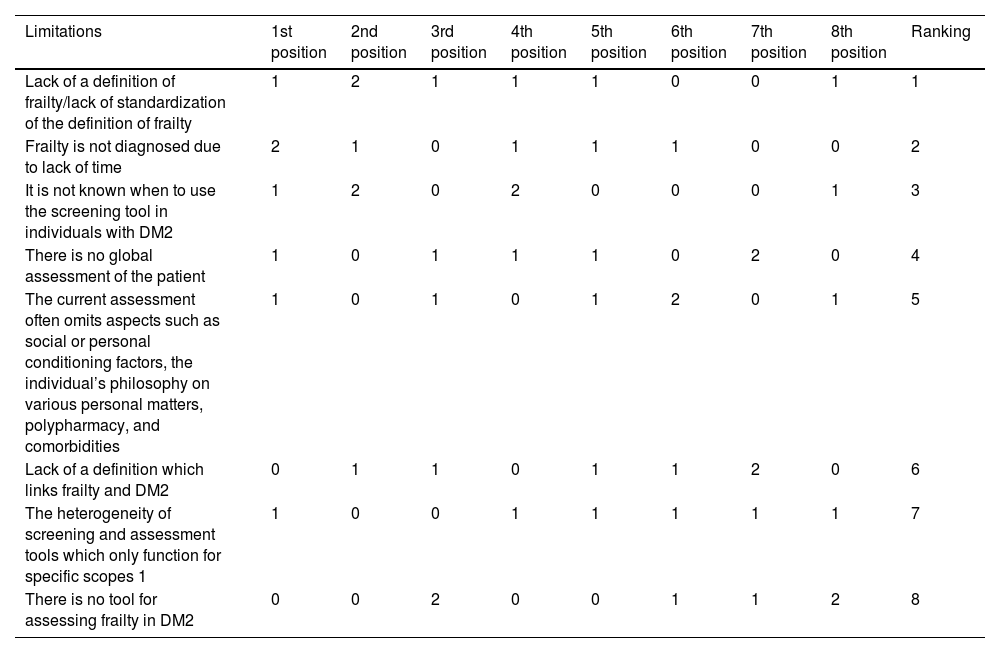
Eight limitations were identified in the assessment of frailty in IWDM2, valued by the SC according to their importance (Table 2). The most important limitation was determined to be “lack of a definition of frailty/lack of standardization of the definition of frailty,” followed by “frailty is not diagnosed due to lack of time,” and “it is not known when to use the screening tool in individuals with DM2.” The least important limitation according to the SC was “there is no tool for evaluating frailty in DM2.”
Limitations of the assessment of frailty in patients with type 2 diabetes mellitus.
| Limitations | 1st position | 2nd position | 3rd position | 4th position | 5th position | 6th position | 7th position | 8th position | Ranking |
|---|---|---|---|---|---|---|---|---|---|
| Lack of a definition of frailty/lack of standardization of the definition of frailty | 1 | 2 | 1 | 1 | 1 | 0 | 0 | 1 | 1 |
| Frailty is not diagnosed due to lack of time | 2 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 2 |
| It is not known when to use the screening tool in individuals with DM2 | 1 | 2 | 0 | 2 | 0 | 0 | 0 | 1 | 3 |
| There is no global assessment of the patient | 1 | 0 | 1 | 1 | 1 | 0 | 2 | 0 | 4 |
| The current assessment often omits aspects such as social or personal conditioning factors, the individual’s philosophy on various personal matters, polypharmacy, and comorbidities | 1 | 0 | 1 | 0 | 1 | 2 | 0 | 1 | 5 |
| Lack of a definition which links frailty and DM2 | 0 | 1 | 1 | 0 | 1 | 1 | 2 | 0 | 6 |
| The heterogeneity of screening and assessment tools which only function for specific scopes 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| There is no tool for assessing frailty in DM2 | 0 | 0 | 2 | 0 | 0 | 1 | 1 | 2 | 8 |
DM2: type 2 diabetes mellitus.
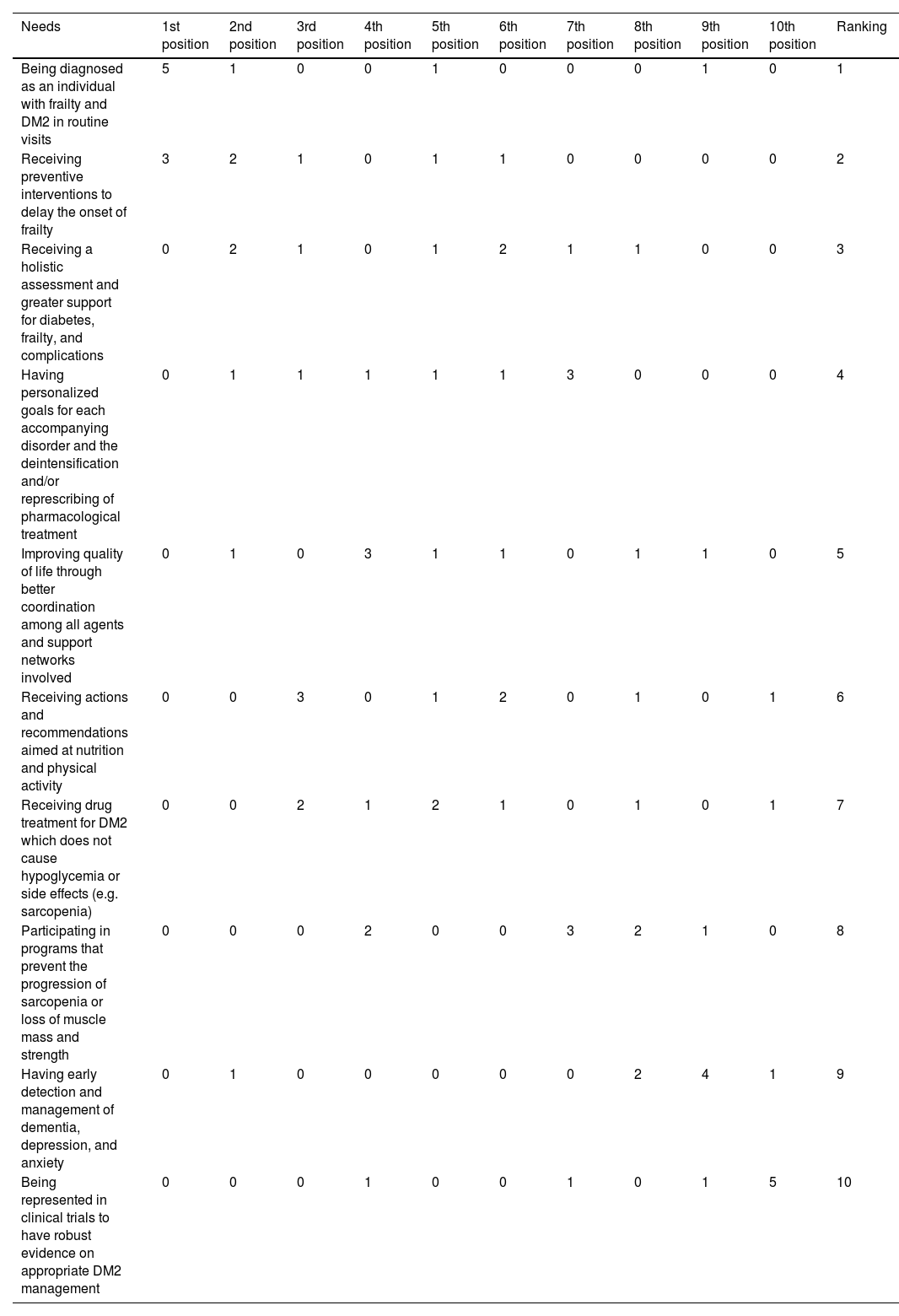
Ten unmet needs of IWDM2 and frailty were detected and evaluated by the SC in terms of importance (see Table 3). The three needs chosen as the most significant were, from greatest to least, “being diagnosed as a individual with frailty and DM2 during routine visits,” “receiving preventive interventions to delay onset of frailty,” and “receive a holistic assessment and greater support for diabetes, frailty, and complications.” The least important needs according to the SC were “being represented in clinical trials to have robust evidence on appropriate DM2 management.”
Unmet needs of individuals with frailty and type 2 diabetes mellitus.
| Needs | 1st position | 2nd position | 3rd position | 4th position | 5th position | 6th position | 7th position | 8th position | 9th position | 10th position | Ranking |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Being diagnosed as an individual with frailty and DM2 in routine visits | 5 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 |
| Receiving preventive interventions to delay the onset of frailty | 3 | 2 | 1 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 2 |
| Receiving a holistic assessment and greater support for diabetes, frailty, and complications | 0 | 2 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 0 | 3 |
| Having personalized goals for each accompanying disorder and the deintensification and/or represcribing of pharmacological treatment | 0 | 1 | 1 | 1 | 1 | 1 | 3 | 0 | 0 | 0 | 4 |
| Improving quality of life through better coordination among all agents and support networks involved | 0 | 1 | 0 | 3 | 1 | 1 | 0 | 1 | 1 | 0 | 5 |
| Receiving actions and recommendations aimed at nutrition and physical activity | 0 | 0 | 3 | 0 | 1 | 2 | 0 | 1 | 0 | 1 | 6 |
| Receiving drug treatment for DM2 which does not cause hypoglycemia or side effects (e.g. sarcopenia) | 0 | 0 | 2 | 1 | 2 | 1 | 0 | 1 | 0 | 1 | 7 |
| Participating in programs that prevent the progression of sarcopenia or loss of muscle mass and strength | 0 | 0 | 0 | 2 | 0 | 0 | 3 | 2 | 1 | 0 | 8 |
| Having early detection and management of dementia, depression, and anxiety | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 2 | 4 | 1 | 9 |
| Being represented in clinical trials to have robust evidence on appropriate DM2 management | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 5 | 10 |
DM2: type 2 diabetes mellitus.
A vote was taken on the usefulness and practicality of the definition of frailty provided by the Ministry of Health for use in IWDM2 (Fig. 2; “Frailty is defined as progressive age-related deterioration of physiological systems that causes a decline in reserves of intrinsic ability, which confers greater vulnerability to stressors and increases the risk of a series of adverse health outcomes.”)22 The mean result of the SC vote was 3.4 (out of 5).

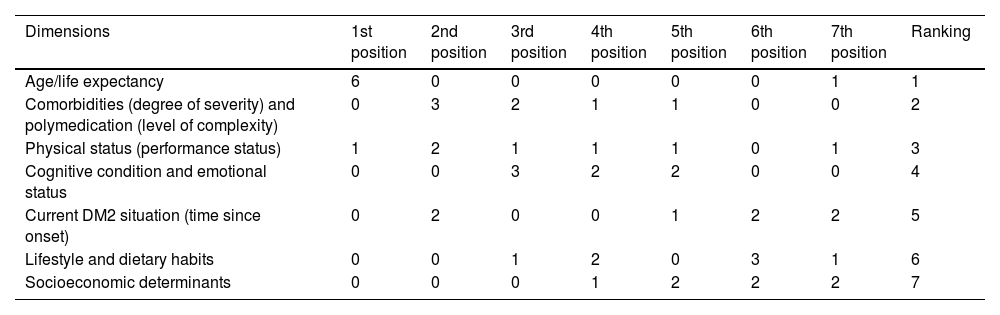
Seven relevant dimensions were identified that should be considered when assessing frailty in a person with DM2. Their assessment, in terms of importance, is shown in Table 4. According to the SC, the most notable dimension was “age/life expectancy,” followed by “comorbidities (degree of severity) and polymedication (level of complexity),” and “physical status (performance status).” On the other hand, “socioeconomic determinants” was considered the least relevant dimension according to the SC.
Dimensions to take into account to evaluate frailty of individuals with type 2 diabetes mellitus according to their relevance.
| Dimensions | 1st position | 2nd position | 3rd position | 4th position | 5th position | 6th position | 7th position | Ranking |
|---|---|---|---|---|---|---|---|---|
| Age/life expectancy | 6 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Comorbidities (degree of severity) and polymedication (level of complexity) | 0 | 3 | 2 | 1 | 1 | 0 | 0 | 2 |
| Physical status (performance status) | 1 | 2 | 1 | 1 | 1 | 0 | 1 | 3 |
| Cognitive condition and emotional status | 0 | 0 | 3 | 2 | 2 | 0 | 0 | 4 |
| Current DM2 situation (time since onset) | 0 | 2 | 0 | 0 | 1 | 2 | 2 | 5 |
| Lifestyle and dietary habits | 0 | 0 | 1 | 2 | 0 | 3 | 1 | 6 |
| Socioeconomic determinants | 0 | 0 | 0 | 1 | 2 | 2 | 2 | 7 |
DM2: type 2 diabetes mellitus.
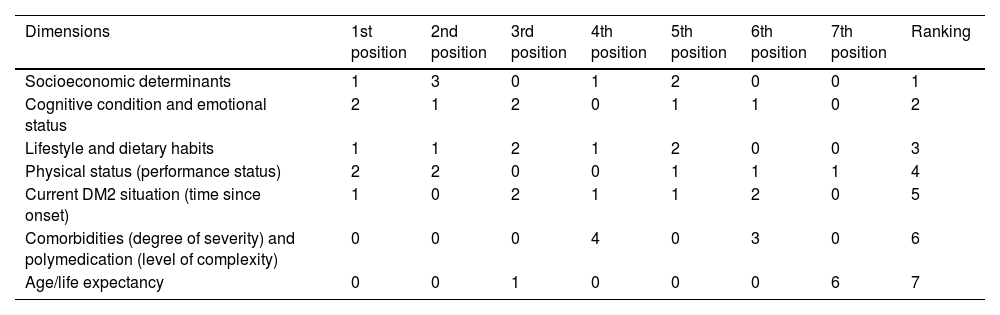
The SC also evaluated the degree of novelty of the dimensions that should be considered when evaluating frailty in IWDM2 (Table 5). The most novel dimensions were “socioeconomic determinants,” followed by “cognitive condition and emotional status,” and “lifestyle and dietary habits,” as options with the next highest ranking. On the other hand, “age/ life expectancy” was considered the least novel dimension.
Dimensions to take into account to evaluate frailty of individuals with type 2 diabetes mellitus according to their novelty.
| Dimensions | 1st position | 2nd position | 3rd position | 4th position | 5th position | 6th position | 7th position | Ranking |
|---|---|---|---|---|---|---|---|---|
| Socioeconomic determinants | 1 | 3 | 0 | 1 | 2 | 0 | 0 | 1 |
| Cognitive condition and emotional status | 2 | 1 | 2 | 0 | 1 | 1 | 0 | 2 |
| Lifestyle and dietary habits | 1 | 1 | 2 | 1 | 2 | 0 | 0 | 3 |
| Physical status (performance status) | 2 | 2 | 0 | 0 | 1 | 1 | 1 | 4 |
| Current DM2 situation (time since onset) | 1 | 0 | 2 | 1 | 1 | 2 | 0 | 5 |
| Comorbidities (degree of severity) and polymedication (level of complexity) | 0 | 0 | 0 | 4 | 0 | 3 | 0 | 6 |
| Age/life expectancy | 0 | 0 | 1 | 0 | 0 | 0 | 6 | 7 |
DM2: type 2 diabetes mellitus.
This study identified the current limitations and needs in the use of the concept of frailty in IWDM2. Eight important limitations in the assessment of frailty in IWDM2 as well as ten unmet needs in the diagnosis and follow-up on this disease were identified and ordered. The definition of frailty in the context of DM2 was also discussed, evaluating the description established by Spain’s Ministry of Health.22 What’s more, seven dimensions were identified that the authors believe should be included in the definition of IWDM2, ordered by importance and by novelty.
Among the limitations of the assessment of frailty in IWDM2, “lack of a definition of frailty/lack of standardization of the definition of frailty” was evaluated as the least important limitation. In light of this opinion, the authors turned to the definition of frailty published by the Spanish Ministry of Health22 for the evaluation of the definition of frailty and assessed the usefulness and practicality of its use in IWDM2. After the vote (mean degree of acceptance of 3.4 out of 5), the authors concluded that this definition focuses solely on functioning and did not establish diagnostic criteria. What’s more, this conceptualization was considered to be complex and difficult to understand, marginalizing other key dimensions of frailty such as sociological and psychological aspects, among others. Therefore, it is believed that the definition of frailty from Spain’s Ministry of Health is not optimal for clinical use in IWDM2,22 although it is a starting point.
Given that there is no definition of frailty that can be used in the clinical management of DM2, this work wanted to be a first step in its creation. Therefore, seven parameters were identified that should be evaluated during routine clinical practice. Among the dimensions defined were “socioeconomic determinants,” “cognitive condition and emotional status,” “lifestyle and dietary habits,” “physical status (performance status),” “current DM2 situation (time since onset),” “comorbidities (degree of severity) and polymedication (level of complexity),” and “age/life expectancy.” A disease-dependent dimension was included among the parameters proposed, namely “current DM2 situation (time since onset),” which sets this definition of frailty apart from other, more general ones. In addition, dimensions that are normally not included in frailty scales were also included and thus were voted as very novel, including “socioeconomic determinants,” “cognitive condition and emotional status,” and “lifestyle and dietary habits.”
It should be remembered that there are two approaches mainly used to characterize frailty in the literature. The first considers frailty as a phenotype of poor physical function, fundamentally supported by two objective measurements: handgrip strength and gait speed (physical frailty). The second approach considers frailty in a much more global manner as the consequence of the cumulative deficit of comorbidities, disability, symptoms, and laboratory data associated with poor outcomes (multidimensional frailty). Therefore, its assessment includes comorbidity and dependence.23 In this sense, the World Health Organization (WHO) defines the terms of intrinsic capacity (IC) and extrinsic factors.24
According to the WHO, IC is a multidimensional health indicator which takes into account crucial mental and physical capacities for individuals to continue leading their lives in a healthy manner.24 The focus agreed upon in this work is multidimensional in nature, in line with what is stated by the WHO. “Cognitive condition and emotional status,” “age and life expectancy,” “comorbidities (degree of severity) and polymedication (level of complexity),” “physical status (performance status),” and “current DM2 situation (time since onset),” can be encompassed under IC described by the WHO whereas “socioeconomic determinants,” and “lifestyle and dietary habits” would be extrinsic factors (Fig. 3). As discussed above, establishing these seven dimensions to define the conceptual framework of frailty in IWDM2 is a first step toward its definition.

This study identified and evaluated limitations in the assessment of individuals with frailty and DM2, concluding that a lack of time and knowledge about the right moment for diagnosis are the second and third most important limitations to its use. The authors believe it is necessary not only to implement a frailty definition and diagnostic tool but also to establish the best time to do so, taking into account the time necessary for diagnosis. In this regard, the FRAIL scale is being used more and more in clinical practice because its five questions can be completed in just a few minutes.25 This scale serves to evaluate frailty in IWDM2, proving to be a useful tool for predicting worsening health.26
Through the debate sparked while conducting this study, ten unmet needs of individuals with frailty and DM2 were identified. The three needs selected as most significant were being diagnosed as a person with frailty during routine visits, receiving preventive interventions which delay onset of frailty, and receiving a holistic evaluation and more support for the disease and its complications. The lack of a definition and diagnostic criteria of frailty in DM2 may be one of the main causes of these limitations. In addition, the holistic treatment of older adults with diabetes is sometimes inadequate and inappropriate because three important elements of IWDM2 are not taken into account. These are the complex management of the disease; the need for an individualized focus in their care; and the assessment of age-related physiology and pharmacology, which increase the risk of adverse drug reactions.27,28
This work has several limitations. First, though the sample size was within the standard range for NGT,29 it was small compared to the number of healthcare professionals involved in managing IWDM2. To address this limitation, a group of experts in different disciplines was used to ensure representation of various areas. However, certain specialties, such as geriatrics, were not included in this study, which limits its perspective. Another limitation is that the experts on the SC work exclusively for Spain’s healthcare system. Therefore, the conclusions of this study may need to be adapted in order to use them in other healthcare systems. Lastly, all meetings were held online, which may increase communication bias, though it also promoted greater participation.30
ConclusionsIn conclusion, this study identified the current limitations and needs in the use of the concept of frailty in IWDM2. Eight limitations and ten unmet needs were determined for individuals with frailty and DM2. The definition of frailty from Spain’s Ministry of Health was evaluated and seven important dimensions for evaluating frailty in IWDM2 were identified. Age is the most important component, but it is followed in order by comorbidities and polymedication, physical status, cognitive and emotional status, current DM2 situation, lifestyle and dietary habits, and socioeconomic determinants. Ideally, all of these dimensions should be evaluated in clinical practice. This article may spark debate in the medical community, improve knowledge on the dimensions that impact frailty in IWDM2, and promote the clinical use of the concept of frailty in IWDM2. A future continuation of this project could involve the creation of an agreed-upon definition of frailty for IWDM2, which would be useful for health professionals and may contribute to improving health outcomes.
FundingMenarini España provided financial support for this work, but had no role in the data collection or analysis or in the creation of this publication.
Conflicts of interestAmparo Marco has received funding from AMGEN, AstraZeneca, Boehringer, Ipsen, Lilly, Novo Nordisk, and Sanofi. Ane Urbina has received funding from AstraZeneca, Boehringer Ingelheim, Esteve, Lilly, Menarini, MSD, and Novo Nordisk. Fernando Gómez-Peralta has received funding from Abbott, AstraZeneca, Boehringer Ingelheim, Bristol-Myers, Insulcloud, Novartis, Novo Nordisk and Sanofi. Laura Romera-Liebana has received funding from AstraZeneca, Boehringer Ingelheim, Lilly, and Menarini. Pilar Cubo-Romano has received funding from Advanz Pharma, Boehringer Ingelheim, Esteve, Faes Farma, Fresenius Kabi, Gebro Farma, Glaxosmithkline, Menarini, Nestle, Novartis and Zambon. Francesc Formiga, Rafael Micó, and José Javier Mediavilla-Bravo have no conflicts of interest.

