


To determine the management of dyslipidemia in primary care after the publication of the American College of Cardiology/American Heart Association (ACC/AHA) 2013 guidelines and Valencian government's algorithm.
MethodWe conducted a cross-sectional descriptive study that employed a survey of primary care physicians of the Community of Valencia between January and October 2016.
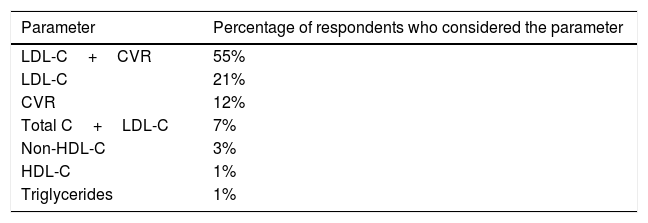
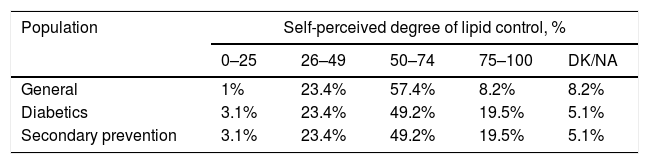
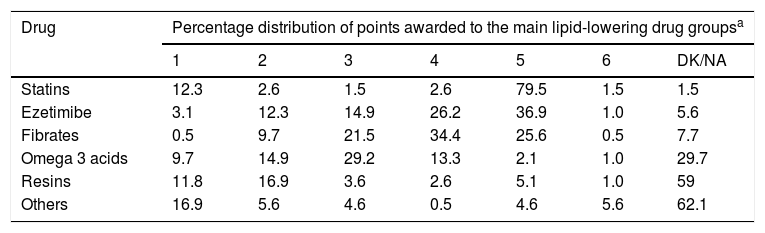
ResultsA total of 199 physicians (mean age, 48.9±11.0 years; experience, 21.3±11.1 years) participated in the survey. The most followed guidelines were those of the European Society of Cardiology (37.5% of respondents) and Valencian government (23.4% of respondents). Some 6.3% of the respondents followed the 2013 ACC/AHA guidelines, and 88.0% established objectives based on LDL cholesterol and cardiovascular risk. The choice of lipid-lowering drug was based on its LDL cholesterol lowering capacity (28.6% of respondents), on the Valencian government's algorithm (23.4%) and on the drug's safety (20.4%). Statins, ezetimibe and fibrates were the preferred hypolipemiant agents, and their combination (51% of respondents) and dosage increases (35%) were the strategies employed for poor control. Lipid profile and transaminase and creatine kinase levels were measured every 6 (59.5%, 52.3% and 54.3% of respondents, respectively) or 12 months (25.1%, 29.2% and 30.3%, respectively). Forty-one percent of the respondents were aware of the controversy surrounding the 2013 ACC/AHA guidelines. Although 60% of the respondents acknowledged its relevance, only 21% changed their daily practices accordingly.
ConclusionsThe Valencian government's algorithm had a greater impact than the 2013 ACC/AHA guidelines in primary care in Valencia. Areas for improvement included the low use of validated guidelines and risk tables and the streamlining of laboratory test periodicity.
Conocer el manejo de la dislipemia en atención primaria tras la publicación de la Guía de la American College of Cardiology/American Heart Association (ACC/AHA) del año 2013 y el algoritmo de la Administración.
MétodoEstudio transversal descriptivo con encuesta a médicos de atención primaria de la Comunidad Valenciana entre enero y octubre de 2016.
ResultadosParticiparon 199 facultativos con una media (desviación típica) de 48,9 (11) años de edad y 21,3 (11,1) años de experiencia. Las guías más seguidas eran las de la European Society of Cardiology (37,5%) y las de la Administración (23,4%). El 6,3% seguía la de la ACC/AHA 2013. El 88% establecía objetivos según colesterol LDL y riesgo cardiovascular. La elección del hipolipemiante estaba basada en su capacidad reductora de colesterol LDL (28,6%), algoritmo de la Administración (23,4%) y seguridad (20,4%). Estatinas, ezetimiba y fibratos eran los hipolipemiantes preferidos, y la combinación (51%) e incremento de dosis (35%) las estrategias en ausencia de control. Se determinaba perfil lipídico, transaminasas y creatincinasa cada 6 (59,5; 52,3 y 54,3%, respectivamente) o 12 meses (25,1; 29,2 y 30,3%, respectivamente). Un 41% era conocedor de la polémica con la Guía ACC/AHA 2013, y aunque un 60% reconocía su relevancia, solo un 21% modificó su quehacer diario por ella.
ConclusionesEl algoritmo de la Administración tuvo mayor impacto que la Guía ACC/AHA 2013 en atención primaria. Campos de mejora fueron el bajo uso de guías y tablas de riesgo validadas, y racionalización de la periodicidad de las analíticas.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


