



To asses if telemedicine with telemonitoring is a clinically useful and safe tool for monitoring patients with COVID-19.
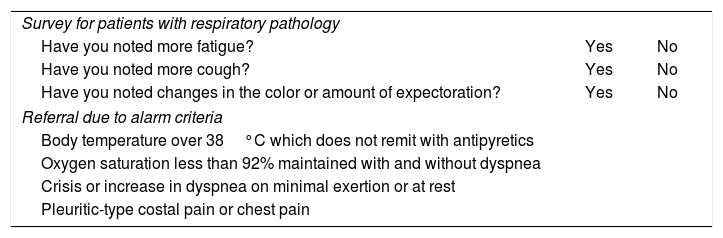
MethodsA prospective observational study of patients with COVID-19 diagnosed via a positive PCR test who were considered high-risk and who were monitored with telemedicine and telemonitoring in the Lugo Healthcare Area between March 17th and April 17th, 2020, was conducted. Two groups of patients were included: those in outpatient monitoring from the beginning and those in outpatient monitoring following hospital discharge. Every patient completed a clinical questionnaire with his or her temperature once per day and oxygen saturation levels three times per day. Proactive monitoring was done by getting in touch with every patient at least once a day.
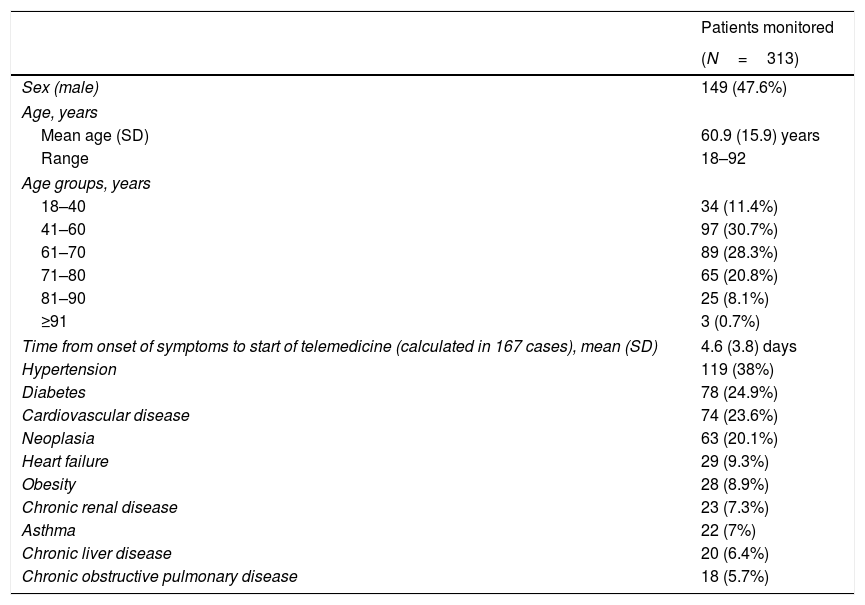
ResultsA total of 313 patients (52.4% female) with a mean age of 60.9 (SD 15.9) years were included. Two patients refused to participate in the program. Finally, 224 were monitored from the beginning and 89 patients were monitored after discharged. In the first group, 38 (16.90%) were referred to the Emergency department on 43 occasions; 18 (8.03%) were hospitalized, and two died. There were no deaths or lifethreatening at home. Including the patients monitored after hospitalization, monitoring was performed in 304 cases. One patient was readmited (0.32%) and another left the program (0.32%). The mean time of monitoring was 11.64 (SD 3.58) days and 224 (73.68%) patients were discharged during the 30 days the study lasted.
ConclusionsOur data suggest that telemedicine with at-home telemonitoring, when used proactively, allows for clinically useful and safe monitoring of high-risk patients with COVID-19.
Evaluar si la telemedicina con telemonitorización es una herramienta clínicamente útil y segura para el seguimiento de pacientes con COVID-19.
MétodosEstudio observacional prospectivo de los pacientes con diagnóstico de COVID-19 por PCR positiva y considerados de alto riesgo que se siguieron con telemedicina y telemonitorización en el Área Sanitaria de Lugo entre el 17 de marzo y el 17 de abril del 2020. Se incluyeron 2 grupos de pacientes: seguimiento ambulatorio desde el inicio y tras el alta hospitalaria. Cada paciente remitió un cuestionario clínico al día con su temperatura y saturación de oxígeno 3 veces al día. El seguimiento fue proactivo, contactando con todos los pacientes al menos una vez al día.
ResultadosSe incluyó a 313 pacientes (52,4% mujeres) con edad media 60,9 (DE 15,9) años. Otros 2 pacientes rehusaron entrar en el programa. Desde el inicio, se siguió ambulatoriamente a 224 pacientes y a 89 pacientes tras su alta hospitalaria. Entre los primeros, 38 (16,90%) se remitieron a Urgencias en 43 ocasiones con 18 (8,03%) ingresos y 2 fallecidos. En los domicilios no hubo fallecimientos ni urgencias vitales. Incluyendo a los pacientes tras hospitalización, el seguimiento se realizó en 304 casos. Un paciente reingresó (0,32%) y otro abandonó (0,32%). El tiempo medio de seguimiento fue 11,64 (DE 3,58) días y en los 30 días del estudio 224 (73,68%) pacientes fueron dados de alta.
ConclusionesNuestros datos sugieren que la telemedicina con telemonitorización domiciliaria, utilizada de forma proactiva, permite un seguimiento clínicamente útil y seguro en pacientes con COVID-19 de alto riesgo.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


