




The incubation period of COVID-19 helps to determine the optimal duration of the quarantine and inform predictive models of incidence curves. Several emerging studies have produced varying results; this systematic review aims to provide a more accurate estimate of the incubation period of COVID-19.
MethodsFor this systematic review, a literature search was conducted using Pubmed, Scopus/EMBASE, and the Cochrane Library databases, covering all observational and experimental studies reporting the incubation period and published from 1 January 2020 to 21 March 2020.We estimated the mean and 95th percentile of the incubation period using meta-analysis, taking into account between-study heterogeneity, and the analysis with moderator variables.
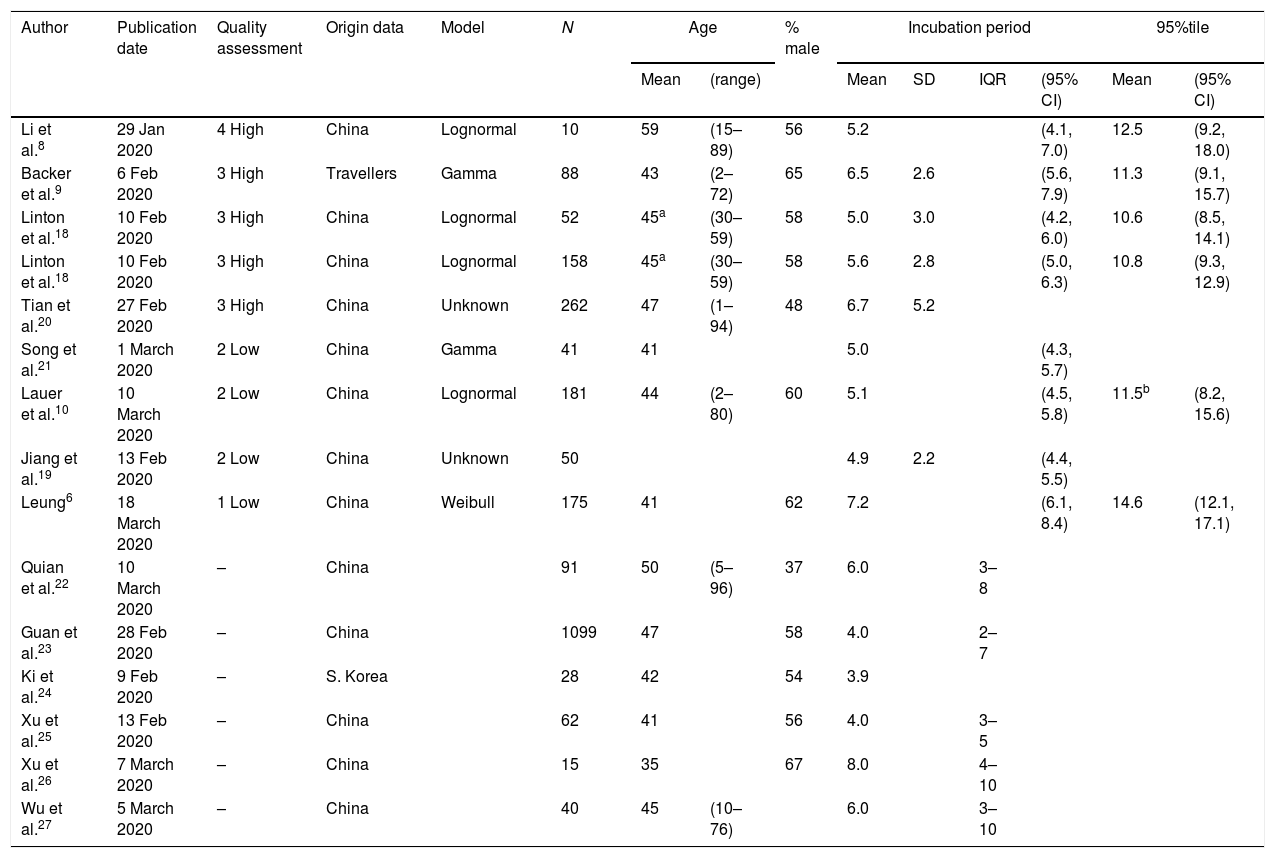
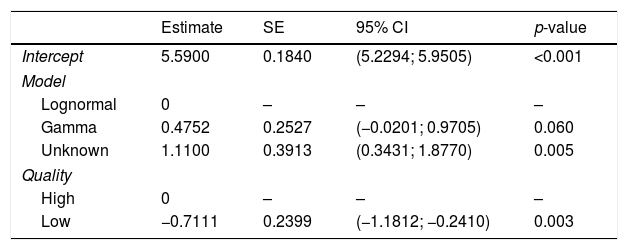
ResultsWe included seven studies (n=792) in the meta-analysis. The heterogeneity (I2 83.0%, p<0.001) was significantly decreased when we included the study quality and the statistical model used as moderator variables (I2 15%). The mean incubation period ranged from 5.6 (95% CI: 5.2–6.0) to 6.7 days (95% CI: 6.0–7.4) according to the statistical model. The 95th percentile was 12.5 days when the mean age of patients was 60 years, increasing 1 day for every 10 years.
ConclusionBased on the published data reporting the incubation period of COVID-19, the mean time between exposure and onset of clinical symptoms depended on the statistical model used, and the 95th percentile depended on the mean age of the patients. It is advisable to record sex and age when collecting data in order to analyze possible differential patterns.
El período de incubación de la COVID-19 ayuda a determinar la duración óptima del período de cuarentena y a crear modelos predictivos de curvas de incidencia. Se han reportado resultados variables en recientes estudios y, por ello, el objetivo de esta revisión sistemática es proporcionar una estimación más precisa del período de incubación de la COVID-19.
MétodosSe realizó una búsqueda bibliográfica en las bases de datos de Pubmed, Scopus/EMBASE y la Cochrane Library, incluyendo todos los estudios observacionales y experimentales que reportaban un período de incubación y que se habían publicado entre el 1 de enero y el 21 de marzo de 2020. Se estimó la media y el percentil 95 del período de incubación mediante metaanálisis, teniendo en cuenta la heterogeneidad entre los estudios y el análisis con variables moderadoras.
ResultadosSe incluyeron siete estudios (n=792) en el metaanálisis. La heterogeneidad (I2 83,0%, p<0,001) disminuyó significativamente cuando se tuvo en cuenta la calidad del estudio y el modelo estadístico utilizado como variables moderadoras (I2 15%). El período medio de incubación oscilaba entre 5,6 (IC 95%: 5,2 a 6,0) y 6,7 días (IC 95%: 6,0 a 7,4), según el modelo estadístico utilizado. El percentil 95 fue de 12,5 días cuando la edad media de los pacientes era de 60 años, aumentando un día por cada 10 años de edad.
ConclusiónSegún los datos publicados sobre el período de incubación de la COVID-19, el tiempo medio entre la exposición y la aparición de los síntomas clínicos depende del modelo estadístico utilizado y el percentil 95, de la edad media de los pacientes. Se recomienda registrar el sexo y la edad en la recogida de los datos para poder analizar los posibles patrones diferenciales.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


