
El papel pronóstico de la presión de pulso (PP) en pacientes con insuficiencia cardiaca (IC) con fracción de eyección de ventrículo izquierdo (FEVI) preservada no es bien conocido. Nuestro objetivo fue evaluarlo en fases de descompensación y de estabilidad.
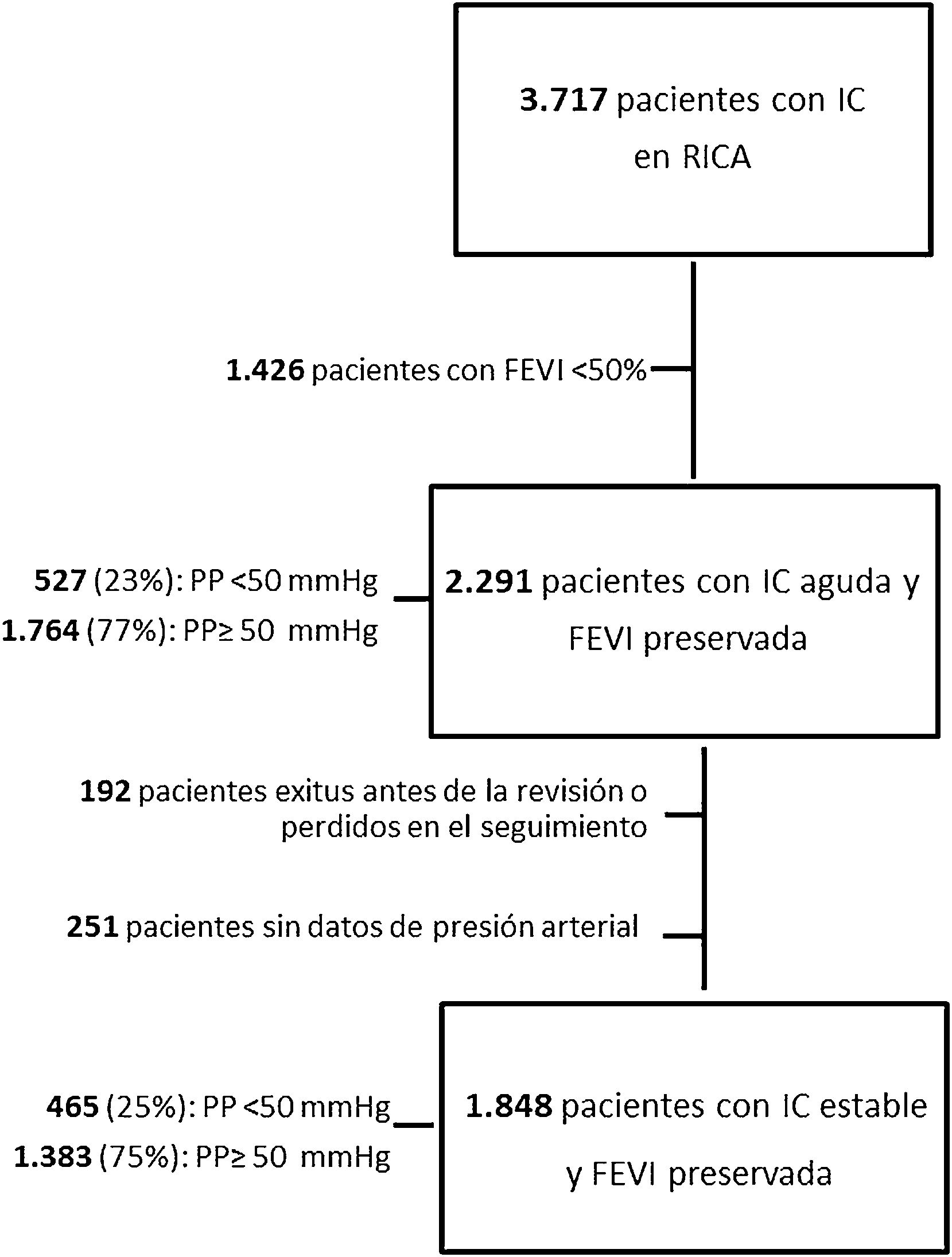
Material y métodosEstudio observacional retrospectivo de pacientes incluidos en el registro RICA entre 2008 y 2021. La presión arterial se recogió al ingreso (descompensación) y a los 3 meses (estabilidad). Se calculó la PP y los pacientes se categorizaron según la PP mayor/igual vs. menor de 50mmHg. Se evaluó la mortalidad por todas las causas al año del ingreso.
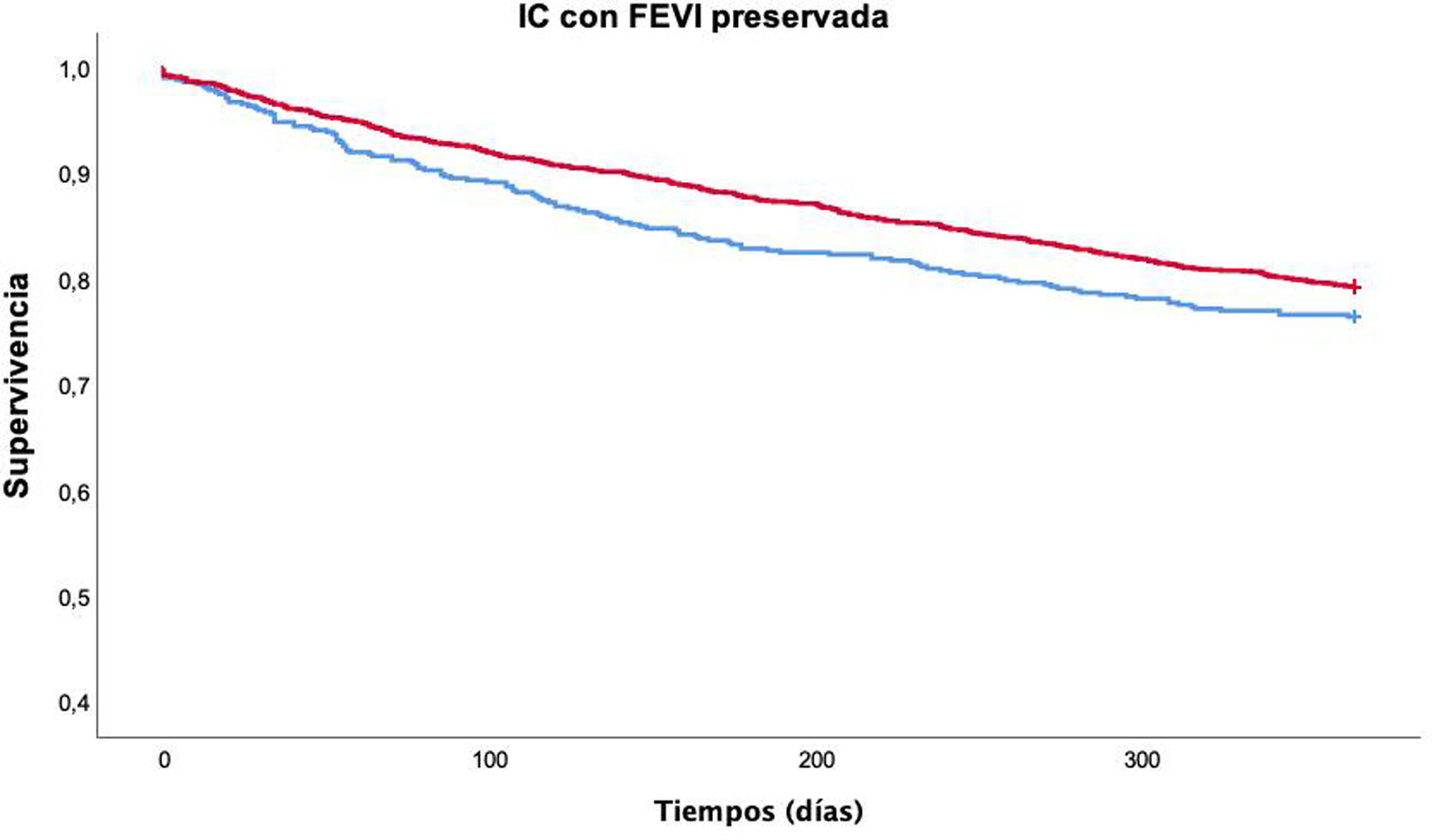
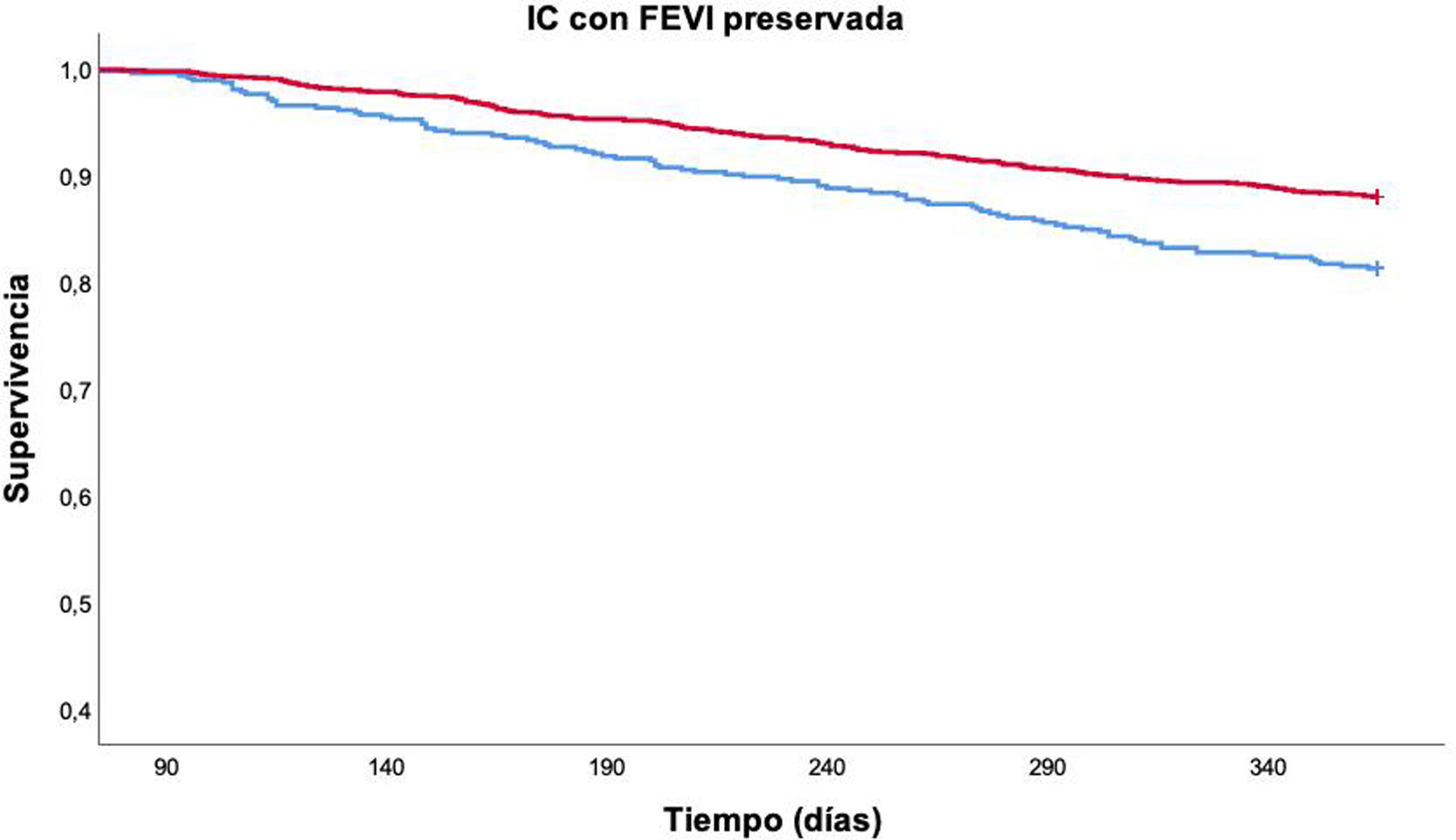
ResultadosSe incluyeron 2.291 pacientes, con edad media 80,1±7,7 años. El 62,9% eran mujeres y un 16,7% tenía antecedentes de cardiopatía isquémica. En fase aguda no hubo diferencias en la mortalidad según los valores de PP, pero en fase estable una PP<50mmHg se asoció de forma independiente con mortalidad por todas las causas al año de seguimiento (HR: 1,57; IC 95%: 1,21-2,05; p=0,001), una vez controlado por edad, sexo, NYHA, IC previa, enfermedad renal crónica, valvulopatía, enfermedad cerebrovascular, Barthel, Pfeiffer, hemoglobina y sodio.
ConclusionesUna PP baja en fase estable se asoció con mayor mortalidad por todas las causas en pacientes con IC con FEVI preservada. Sin embargo, la PP no demostró ser un factor pronóstico en fase de descompensación. Se necesitan más estudios que valoren la relación de esta variable con la mortalidad en los pacientes con IC.
The prognostic role of pulse pressure (PP) in patients with heart failure (HF) with preserved left ventricular ejection fraction (LVEF) is not well understood. This study aimed to evaluate it in acute and stable HF.
Material and methodsThis work is a retrospective observational study of patients included in the RICA registry between 2008 and 2021. Blood pressure was collected on admission (decompensation) and at three months (stability). PP was calculated and patients were categorized according to whether PP was greater than/equal to or less than 50mmHg. All-cause mortality at one year after admission was assessed.
ResultsA total of 2,291 patients were included. The mean age was 80.1±7.7 years, 62.9% were women, and 16.7% had a history of ischemic heart disease. In the acute phase, there were no differences in mortality according to PP values, but in the stable phase, PP <50mmHg was independently associated with all-cause mortality at one year (HR 1.57, 95% CI 1.21-2.05, p=0.001) after adjusting for age, sex, New York Heart Association functional class, previous HF, chronic kidney disease, valvular heart disease, cerebrovascular disease, score on the Barthel and Pfeiffer scales, and hemoglobin and sodium levels.
ConclusionsLow stable-phase PP was associated with increased all-cause mortality in HF patients with preserved LVEF. However, PP was not found to be a prognostic facture in the acute phase. Further studies are needed to assess the relationship of this variable with mortality in HF patients.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


