



Recent surgery is a well-known major transient risk factor for venous thromboembolism (VTE) due to the low risk of VTE recurrence after anticoagulation is discontinued. On the other hand, the risk of VTE recurrence among patients with COVID-19-associated VTE is unknown. This study aimed to compare the risk of VTE recurrence between patients with COVID-19- and surgery-associated VTE.
MethodsA prospective observational single-center study was performed including consecutive patients diagnosed with VTE in a tertiary hospital from January 2020 to May 2022 and followed up for at least 90 days. Baseline characteristics, clinical presentation, and outcomes were assessed. The incidence of VTE recurrence, bleeding, and death was compared between both groups.
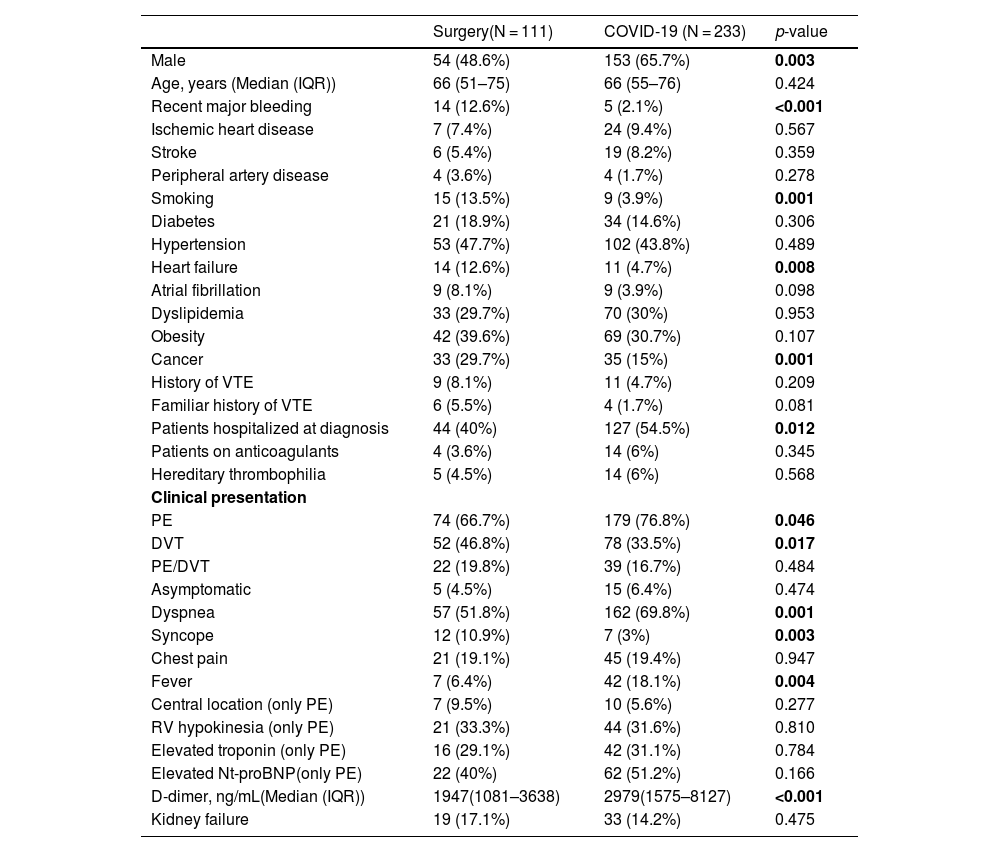
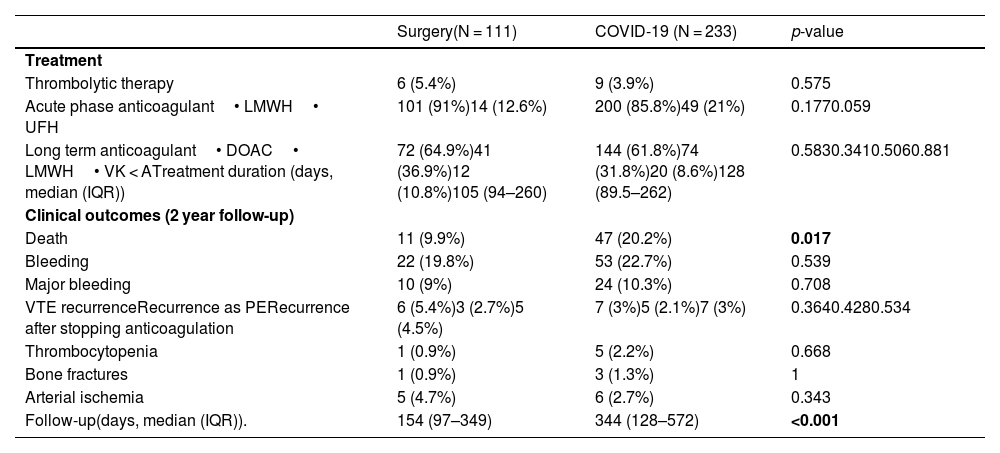
ResultsA total of 344 patients were included in the study: 111 patients with surgery-associated VTE and 233 patients with COVID-19-associated VTE. Patients with COVID-19-associated VTE were more frequently men (65.7% vs 48.6%, p = 0.003). VTE recurrence was 3% among COVID-19 patients and 5.4% among surgical patients, with no significant differences (p = 0.364). The incidence rate of recurrent VTE was 1.25 per 1000 person-months in COVID-19 patients and 2.29 person-months in surgical patients, without significant differences (p = 0.29). In the multivariate analysis, COVID-19 was associated with higher mortality (HR 2.34; 95% CI 1.19–4.58), but not with a higher risk of recurrence (HR 0.52; 95% CI 0.17–1.61). No differences were found in recurrence in the multivariate competing risk analysis (SHR 0.82; 95% CI 0.40–2.05).
ConclusionsIn patients with COVID-19 and surgery-associated VTE, the risk of recurrence was low, with no differences between both groups.
La cirugía reciente es un importante factor de riesgo transitorio bien conocido para tromboembolismo venoso (TEV) debido al bajo riesgo de recurrencia de TEV después de suspender la anticoagulación. Por otro lado, se desconoce el riesgo de recurrencia de TEV entre pacientes con TEV asociado a COVID-19. Este estudio tuvo como objetivo comparar el riesgo de recurrencia de TEV entre pacientes con TEV asociado a cirugía y COVID-19.
MétodosSe realizó un estudio prospectivo observacional unicéntrico que incluyó pacientes consecutivos diagnosticados de TEV en un hospital terciario desde enero de 2020 hasta mayo de 2022 y seguidos durante al menos 90 días. Se evaluaron las características iniciales, la presentación clínica y los resultados. Se comparó la incidencia de recurrencia de TEV, hemorragia y muerte entre ambos grupos.
ResultadosSe incluyeron en el estudio un total de 344 pacientes: 111 pacientes con TEV asociada a cirugía y 233 pacientes con TEV asociada a COVID-19. Los pacientes con TEV asociada a COVID-19 fueron con mayor frecuencia hombres (65,7% vs 48,6%, p = 0,003). La recurrencia de TEV fue del 3% entre los pacientes con COVID-19 y del 5,4% entre los pacientes quirúrgicos, sin diferencias significativas (p = 0,364). La tasa de incidencia de TEV recurrente fue de 1,25 por 1000 personas-mes en pacientes con COVID-19 y de 2,29 personas-mes en pacientes quirúrgicos, sin diferencias significativas (p = 0,29). En el análisis multivariado, la COVID-19 se asoció con mayor mortalidad (HR 2,34; IC 95% 1,19-4,58), pero no con mayor riesgo de recurrencia (HR 0,52; IC 95% 0,17−1,61). No se encontraron diferencias en la recurrencia en el análisis multivariado de riesgos competitivos (SHR 0,82; IC 95% 0,40 – 2,05).
ConclusionesEn pacientes con COVID-19 y TEV asociada a cirugía, el riesgo de recurrencia fue bajo, sin diferencias entre ambos grupos.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


