
Información del artículo
Texto completo
Bibliografía
Descargar PDF
Estadísticas
Tablas (1)
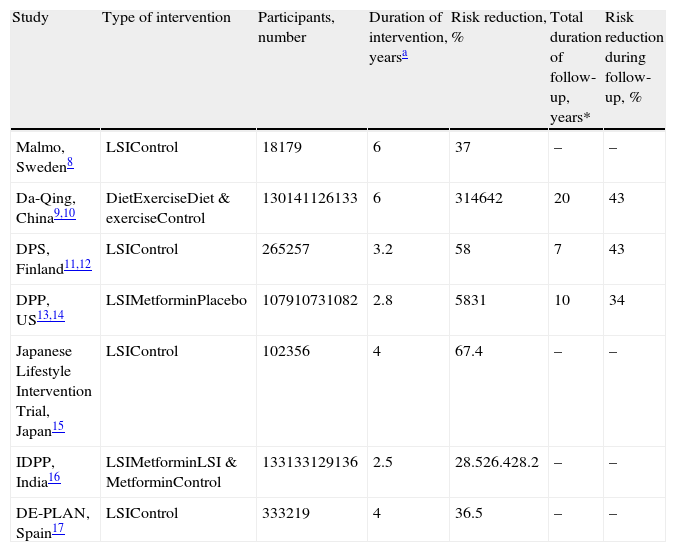
Table 1. Summary of randomized clinical trials of primary prevention of type 2 diabetes.
Artículo
Opciones para acceder a los textos completos de la publicación Revista Clínica Española
Socio
Si es usted socio de FESEMI siga los siguientes pasos:
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<

Comprar