



Coronavirus disease 2019 (COVID-19), caused by SARS-CoV-2 infection, spreads swiftly in nursing homes and assisted living facilities, leading to a high degree of lethality. The data generated by an epidemiological surveillance program allow for obtaining valid information on the diseases’ epidemiology and possible prevention methods.
ObjectiveThis work aims to analyze COVID-19 epidemiology among healthcare staff based in the Seville healthcare district (Spain) and evaluate its role in outbreaks in nursing homes.
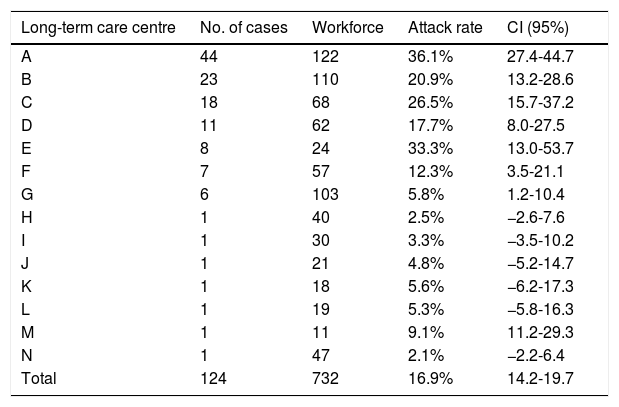
MethodsThis is an observational, descriptive study of 88 assisted living facilities located in the city of Seville from March 1 to May 23, 2020. Data were obtained via epidemiological surveys on staff at centers where there were outbreaks (n = 732 in 14 nursing homes). The cumulative incidence, epidemic curves, sociodemographic and clinical characteristics, and delays in isolation and notification of cases were calculated. For the statistical analysis, measures of central tendency and dispersion were used as well as confidence intervals and statistical hypothesis tests.
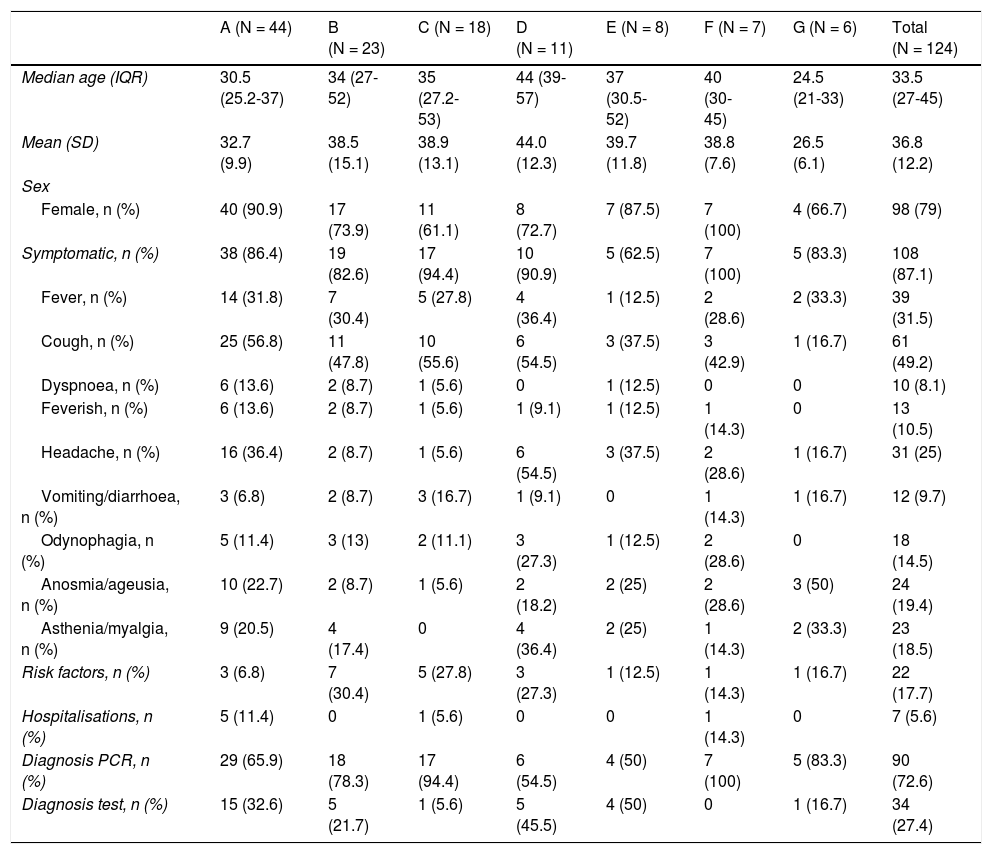
ResultsThere were 124 cases in staff members (cumulative incidence 16.9%), 79.0% of which were in women. The majority presented with mild symptoms (87.1%). The most common symptoms were fever (31.5%) and cough (49.2%). The median number of days from onset of symptoms to isolation was three.
ConclusionsA high incidence in nursing home staff along with delays in isolation were observed, which could affect the dynamics of transmission in outbreaks. It is necessary to review disease identification and isolation practices among staff as well as emphasize rapid implementation of prevention measures.
La infección por coronavirus SARS-CoV-2 se transmite rápidamente en residencias de mayores y centros sociosanitarios, provocando una elevada letalidad. Los datos generados por el programa de vigilancia epidemiológica permiten información válida sobre la epidemiología del problema y las posibilidades de prevención.
ObjetivoAnalizar la epidemiología de la infección por COVID-19 entre los profesionales sociosanitarios del Distrito Sanitario Sevilla y su papel en la evolución de los brotes en las residencias de mayores.
MetodologíaEstudio sobre 88 centros sociosanitarios de la ciudad de Sevilla en el período del 1 marzo al 23 mayo de 2020, partiendo de las encuestas epidemiológicas en casos del personal donde hubo brotes (n = 732 en 14 residencias). Se calcularon incidencias acumuladas, curvas epidémicas, características sociodemográficas y clínicas, y demoras en el aislamiento y notificación de los casos. Para el análisis estadístico se emplearon medidas de tendencia central y de dispersión, así como intervalos de confianza y pruebas de contraste de hipótesis.
ResultadosSe produjeron 124 casos en trabajadores (tasa de ataque 16,9%), 79,0% en mujeres. La gran mayoría presentaron síntomas leves (87,1%). Los comunes fueron fiebre (31,5%) y tos (49,2%). La mediana de días desde el inicio de los síntomas hasta el aislamiento fue 3 días.
ConclusionesSe objetiva una elevada incidencia en el personal sociosanitario con demoras en el aislamiento que pudieron condicionar la dinámica de transmisión en los brotes. Es necesario revisar las prácticas de identificación de la enfermedad y el aislamiento entre el personal, énfasis en la implementación rápida de medidas de prevención.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


