
AL amyloidosis is a rare condition whose management is undergoing changes due to recent advances in diagnosis and treatment. We describe a contemporary series of patients with AL amyloidosis to analyze the features that enable early diagnosis and optimal management.
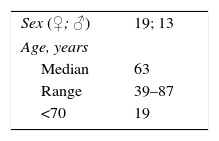
Patients and methodsWe recruited for analysis 32 patients (19 women; mean age, 63 years) treated consecutively at our center.
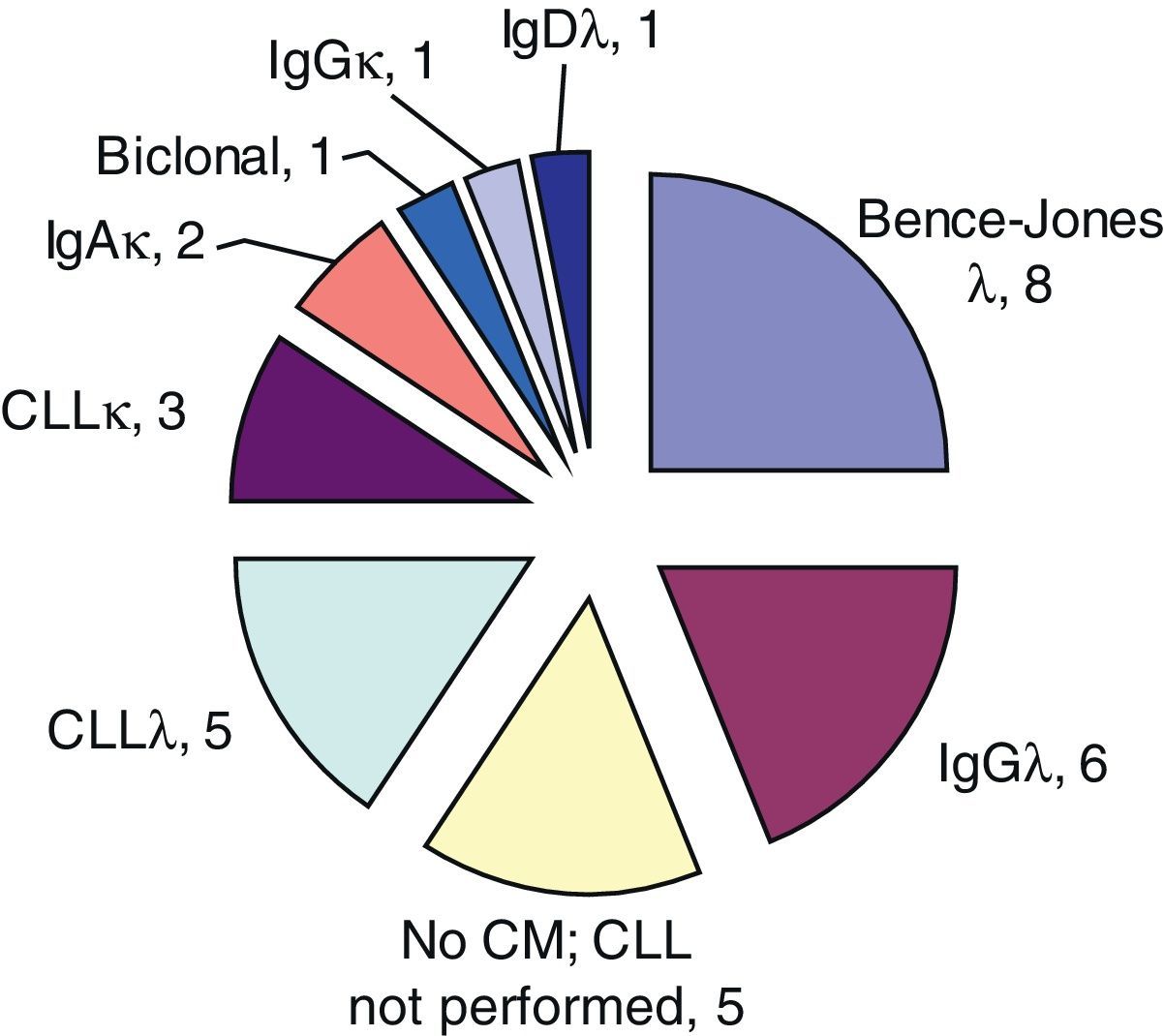
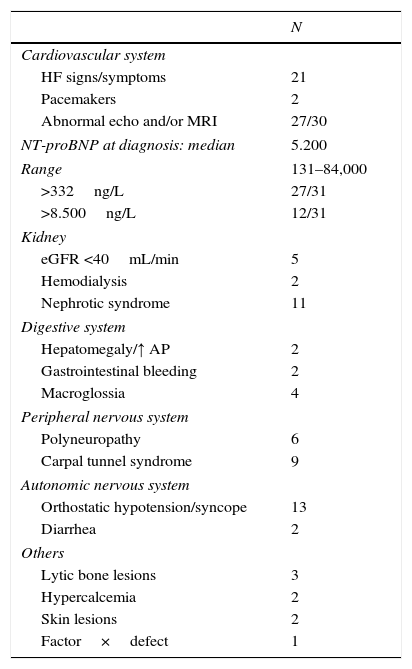
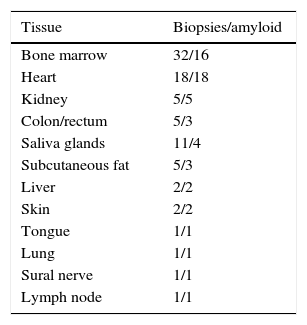
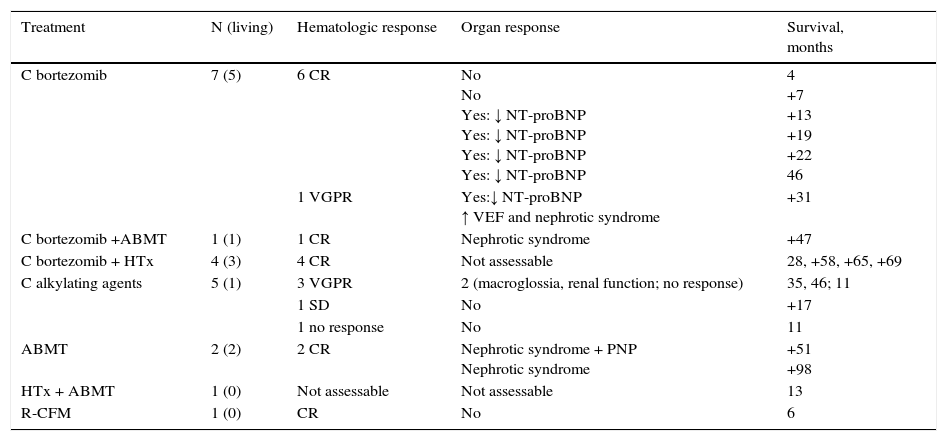
ResultsEighty-four percent of the patients presented with asthenia, dyspnea or edema, with a previous duration of symptoms of 8 months (median). Cardiac (21/32) and renal impairment were the most common type (11/32). All of the patients, except one, had a monoclonal component in serum/urine or abnormal values for free light chains (78%, λ). The bone marrow (BM) showed clonal plasmacytosis in 29 cases. All of the cardiac biopsies and 50% of the BM biopsies showed amyloid deposits. The results of the echocardiogram and/or cardiac resonance were abnormal in 27/30 cases. The median NT-proBNP value at diagnosis was 5200ng/ml. Thirteen patients died due to heart failure, 2 due to rejection after heart transplantation, 2 due to pneumonia and 1 after a stroke. Ten patients did not undergo treatment, 12 were treated with bortezomib and 5 were treated with alkylating agents. Five patients underwent heart transplantation and 4 underwent autologous bone marrow transplantation. Fourteen patients achieved a complete hematologic response and 10 achieved organ response. The median survival was 17 months.
ConclusionsCardiac involvement is the major determinant of prognosis. Yield of involved organ biopsy is high (100% heart biopsies). Antineoplastic treatment with bortezomib and/or autologous bone marrow transplantation achieves hematological responses with improvements in organ impairment.
La amiloidosis AL es una entidad rara cuyo manejo está cambiando gracias a avances recientes en el diagnóstico y tratamiento. Describimos una serie contemporánea de enfermos con amiloidosis AL, para analizar aspectos que permiten un diagnóstico precoz y un manejo óptimo.
Pacientes y métodosHemos reunido para su análisis 32 pacientes (19 mujeres, edad mediana 63 años) atendidos consecutivamente en nuestro centro.
ResultadosEl 84% de los enfermos comenzaron con astenia, disnea o edemas con una duración previa de los síntomas de 8 meses (mediana). La afectación cardiaca (21/32) y la renal fueron las más frecuentes (11/32). Todos los enfermos, excepto uno, presentaban componente monoclonal en suero/orina o valores anormales de cadenas ligeras libres (78%, λ). La médula ósea (MO) mostraba plasmocitosis clonal en 29 casos. El 100% de las biopsias cardiacas y el 50% de las de MO mostraron amiloide. El ecocardiograma y/o la resonancia cardiaca fueron anormales en 27/30 casos. La mediana de NT-proBNP al diagnóstico fue de 5200ng/mL. Trece enfermos fallecieron por insuficiencia cardiaca, 2 por rechazo tras trasplante cardiaco, 2 por neumonía y uno tras ictus. Diez enfermos no recibieron tratamiento; 12 recibieron bortezomib y 5 alquilantes. Cinco enfermos recibieron un trasplante cardiaco y 4, un autotrasplante de MO. Catorce enfermos alcanzaron respuesta hematológica completa y 10, respuesta de órganos. La supervivencia mediana fue de 17 meses.
ConclusionesLa afectación cardiaca es el principal determinante pronóstico. La rentabilidad de las biopsias de órganos afectados es alta (100% biopsias cardiacas). El tratamiento antineoplásico con bortezomib y/o autotrasplante de MO consigue respuestas hematológicas con mejoría de la afectación de órganos.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


